TC/EC Sample and Distribution Chlorine Submission Guide
Excel Reporting
This page outlines how to report Routine, Repeat, and Special Total Coliform (TC) and E.coli (EC) samples collected from distribution system for RTCR (Revised Total Coliform Rule), Triggered source water samples collected at well for GWR (Ground Water Rule), and distribution chlorine field results (if reported).
The guidance is separated into three sections to match the sections in the CMDP Excel template. This includes general Sample Information, Microbial Results, and Field Results and Measurements (for reporting distribution chlorine). Additionally, this page includes a link to the Methods Chart and examples of completed sample submissions.
This guidance page notes the state/federally required fields within each section. Submit the information as described. Do not rely on the symbols noted on the template, as they do not include the state required fields.
If you have questions, please contact DEC CMDP support staff at dec.cmdpsupport@alaska.gov.
Fields with one asterisk (*) are required to meet federal and state reporting requirements. Fields with two asterisks (**) are conditionally or situationally required. The remaining fields are not required for a successful data submission. Samples will be rejected if required fields are left blank.
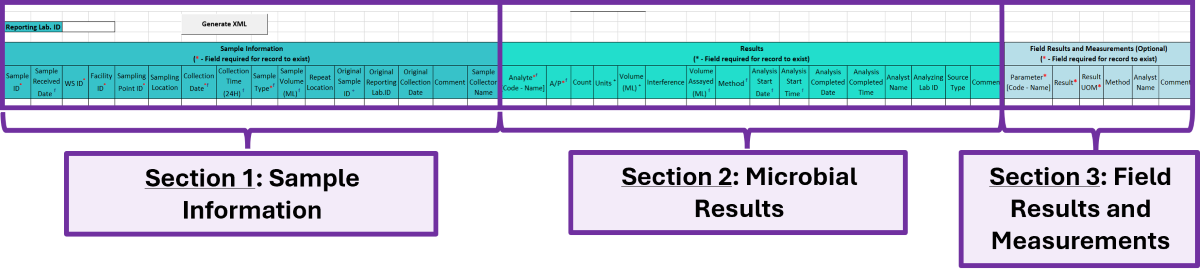
Section 1: Sample Information
- Reporting Lab. ID*: Lab identification number.
- Sample ID*: Lab sample identification number, limit to 20 characters (numbers, letters, dash/underscore are allowed).
- Sample Received Date*: Date sample was received by lab (MM/DD/YY).
- WS ID*: Public Water System identification number (PWSID).
- NOTE: Each water system name has a unique PWSID number. If the name and number on the work order does not match what is listed in CMDP, investigate to ensure accuracy and consistency.
- Facility ID*: Select the appropriate water system facility from where the sample was collected.
- Sampling Point ID*: Select the appropriate sample point related to the facility where the sample was collected.
- If you are unsure of the Facility ID or Sample Point ID to enter, review the How to find PWS Facility ID/Sample Point ID information page.
- Sampling Location*: This field must describe the location where the sample was taken from in the distribution system (i.e., 123 Main Street, Health Clinic, Kitchen sink, etc.). Keep description succinct (numbers, letters, dash/underscore only).
- Collection Date*: Date sample collected (MM/DD/YY).
- Collection Time (24H)*: Time sample collected (HH:MM).
- Sample Type*: From the drop down menu (pictured below), select the appropriate sample type (i.e., routine, repeat, special, triggered, etc.).
- NOTE: If you are submitting a sample that is Not For Compliance, select Special from the Sample Type drop down menu.
- Sample Volume*: Volume of sample analyzed (numerical value only).
- Repeat Location: Not required but report if information if available.
- Original Sample ID**: If reporting a Repeat or Triggered sample, enter the lab Sample ID of the original TC+ sample that caused the repeat or triggered sample(s) to be collected.
- Original Reporting Lab. ID: Not required but report if information if available.
- Original Collection Date: Not required but report if information if available (MM/DD/YY).
- Comment: Not required, however if comments are provided, please limit characters to numbers, letters, dash or underscore. In particular, do NOT include quotation marks.
- Sample Collector Name: Name of sample collector, report if information is provided.
Section 2: Microbial Results
- Analyte [Code-Name]*: From the drop down menu, select 3100 Coliform (TCR) or 3014 E. Coli, as appropriate.
- Reminder: EC speciation is required for TC Present samples. For TC Absent samples, it is not required.
- A/P*: From the drop down menu, select whether the contaminant was Present or Absent in the analyzed sample.
- Count**: Count of TC+ or EC+ sample. Enter the count only if required by analysis method.
- Units**: From the drop down menu, select the unit of measure for the sample result as appropriate.
- Volume**:Volume of sample. Enter the appropriate volume of the TC+/EC+ sample only if required by the analysis method.
- Interference: Not required but report if applicable.
- Volume Assayed*: Volume of sample analyzed (numerical value only).
- Method*: This drop-down menu includes ALL microbial analyses methods and is NOT filtered by the analytes your lab (or subcontracting lab) is certified for. Be sure to verify certification status and select the appropriate method. If the method is reported incorrectly, it will be rejected from the state database.
- If you are unsure which method should be reported, please see the Methods Chart to determine correct reporting.
- Analysis Start Date*: Date when lab began analysis (MM/DD/YY).
- Analysis Start Time*: Time when lab began analysis (HH:MM).
- Analysis Completed Date: Not required but report if information is available (MM/DD/YY).
- Analysis Completed Time: Not required but report if information is available (HH:MM).
- Analyst Name: Not required but report if information is available.
- Analyzing Lab ID**: If the sample was subcontracted to a different lab for analysis, the analyzing lab identification number is required to be reported here.
- Source Type: Not required but report if information is available.
- Comment: Not required, however if comments are provided, please limit characters to numbers, letters, dash or underscore. In particular, do NOT include quotation marks.
Section 3: Field Results and Measurements (Distribution Chlorine)
For systems that report a distribution chlorine residual along with their routine Total Coliform sample, please report the information in this section.
- Parameter [Code-Name]*: From the drop down menu, select the appropriate parameter analyzed, either 1013-FreeChlorineResidual or 1012-TotalChlorineResidual depending on what is noted on the COC. If the type is not noted on the COC, use the Free Chlorine Residual.
- Result*: Enter the numerical value of the field result/measurement.
- Result UOM*: From the drop down menu, select the appropriate unit of measurement for the parameter.
- Method: Do NOT report data in this field.
- Analyst Name: Not required.
- Comment: Not required, however if comments are provided, please limit characters to numbers, letters, dash or underscore. In particular, do NOT include quotation marks.
Section 4: Examples
Excel Examples Document - This document includes several examples as follows:
- Tab 1 - Routine Sample TC Absent with distribution chlorine
- Tab 2 - Routine Sample TC Present / EC Absent without distribution chlorine
- Tab 3 - Routine Sample TC Present / EC Present with distribution chlorine
- Tab 4 - Repeat Sample TC Absent
- Tab 5 - Triggered Sample TC Absent
- Tab 6 - Special Sample TC Absent
 Indicates an external site.
Indicates an external site.